Every billable code the chart supports — proven.
Capsa Charge Capture reads the signed ambulatory note, recommends the CPT/HCPCS codes it supports with a plain-English reason, and verifies every quote is verbatim in the chart before a coder sees it — then scores itself against what your coders actually billed.
Both ways coding goes wrong are expensive.
After a provider signs a note, a coder reads it and bills every service performed. Billable work is easy to miss, inconsistent between coders, and hard to audit after the fact.
Lost, compliant revenue — gone for good
Billable work the coder didn't capture is money you earned and won't see. At scale, a few missed codes per visit is a seven-figure annual leak.
Audit risk and clawback exposure
Codes billed without support in the chart invite denials and recoupment. The goal isn't “more billing” — it's the right amount, provably.
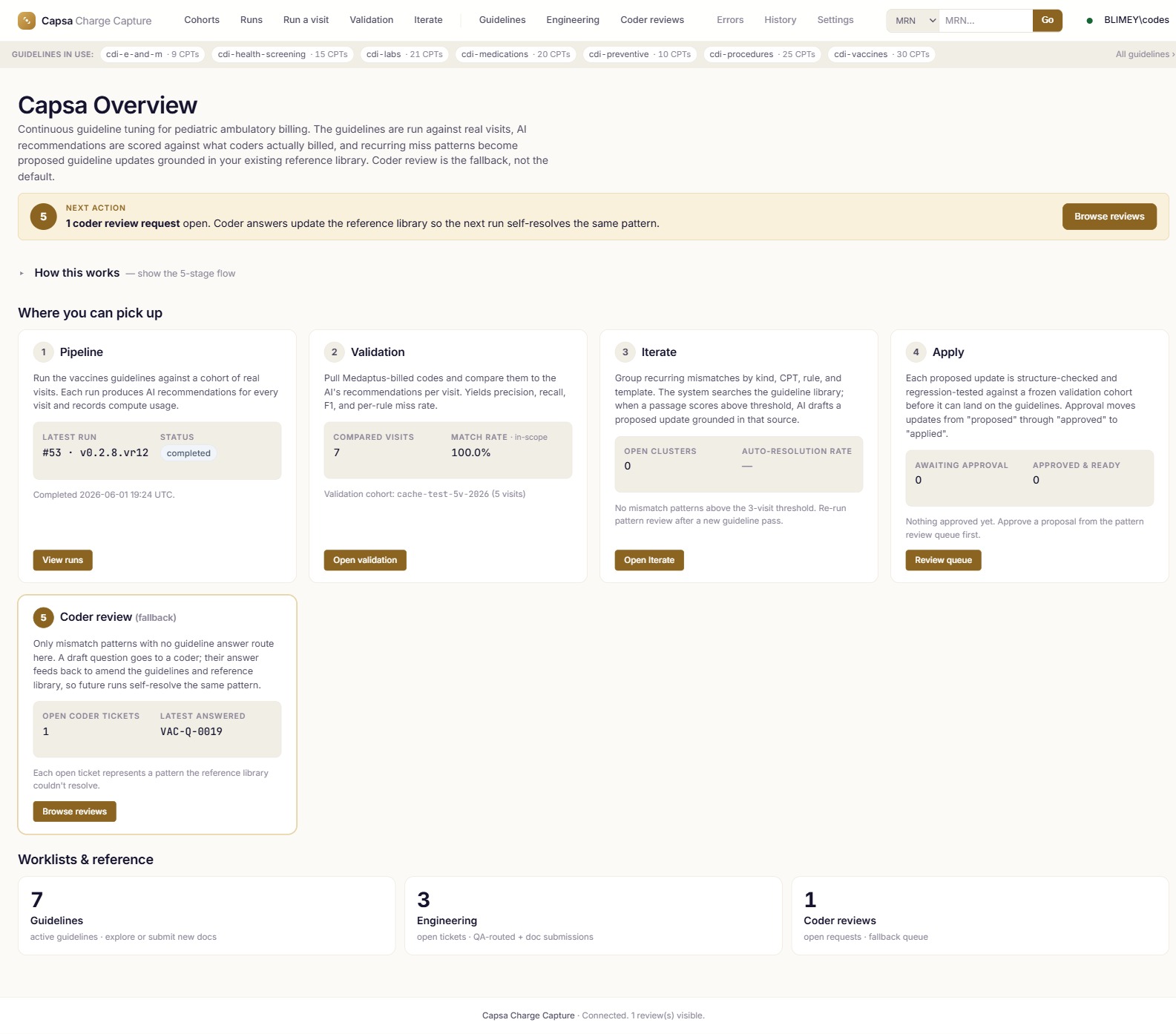
Read the note. Prove the code. Measure against what was billed.
Ingest
The signed note comes in from the EHR; augmenters fill known gaps like structured vaccine records.
Triage
A fast model decides which coding categories even apply, so effort goes only where it's needed.
Analyze
Each category runs an explicit, human-readable rule set and proposes codes with a plain-English reason.
Cite-check
Every quote is verified verbatim in the chart. Unsupported recommendations are dropped before a coder sees them.
Validate
Predictions are scored against what the coder actually billed — scope-aware precision and recall.
Real screens from the product.
Screenshots are from the live application. Patient identifiers and clinical text are scrubbed; codes, rules, versions, and metrics are real.
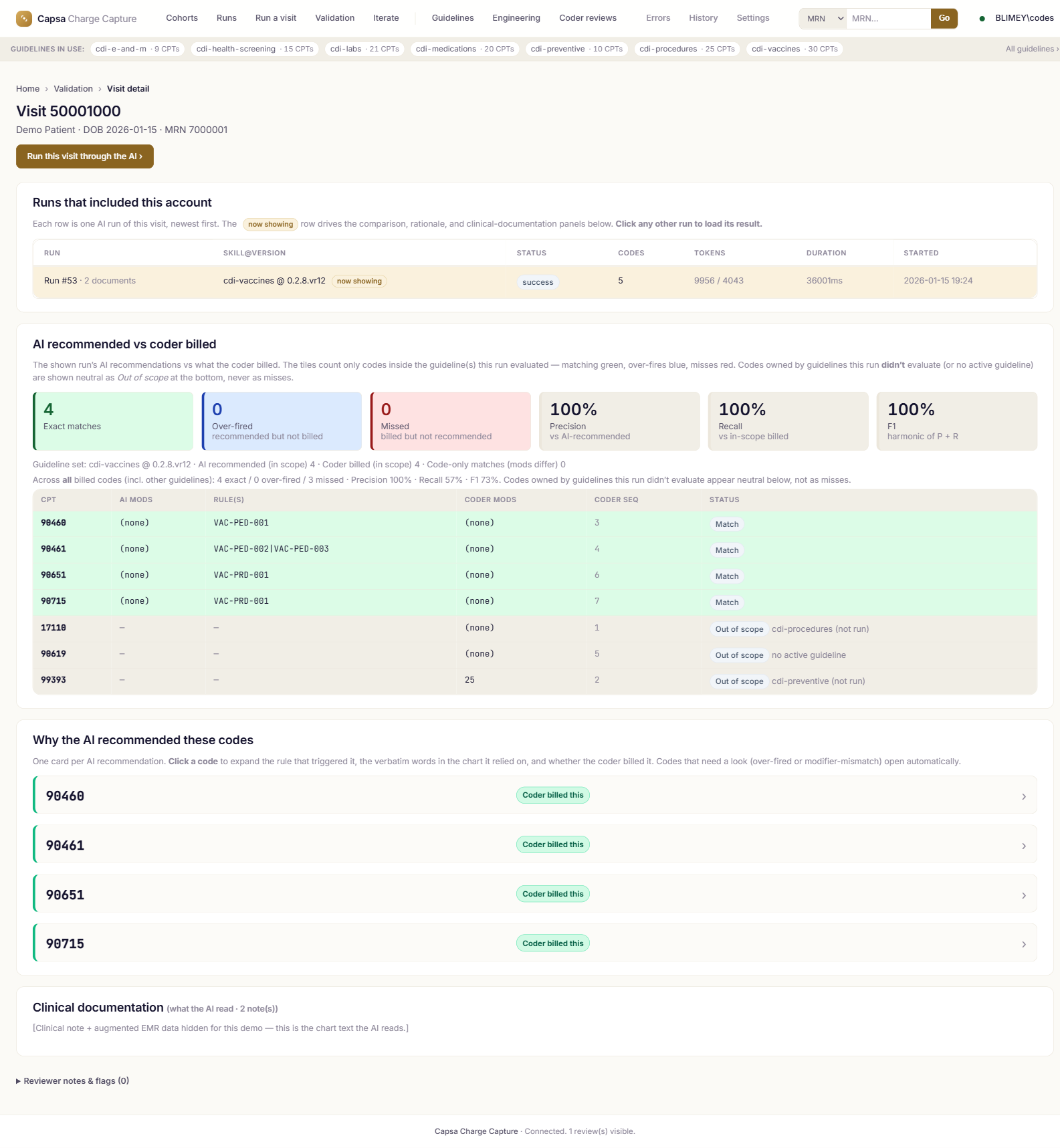
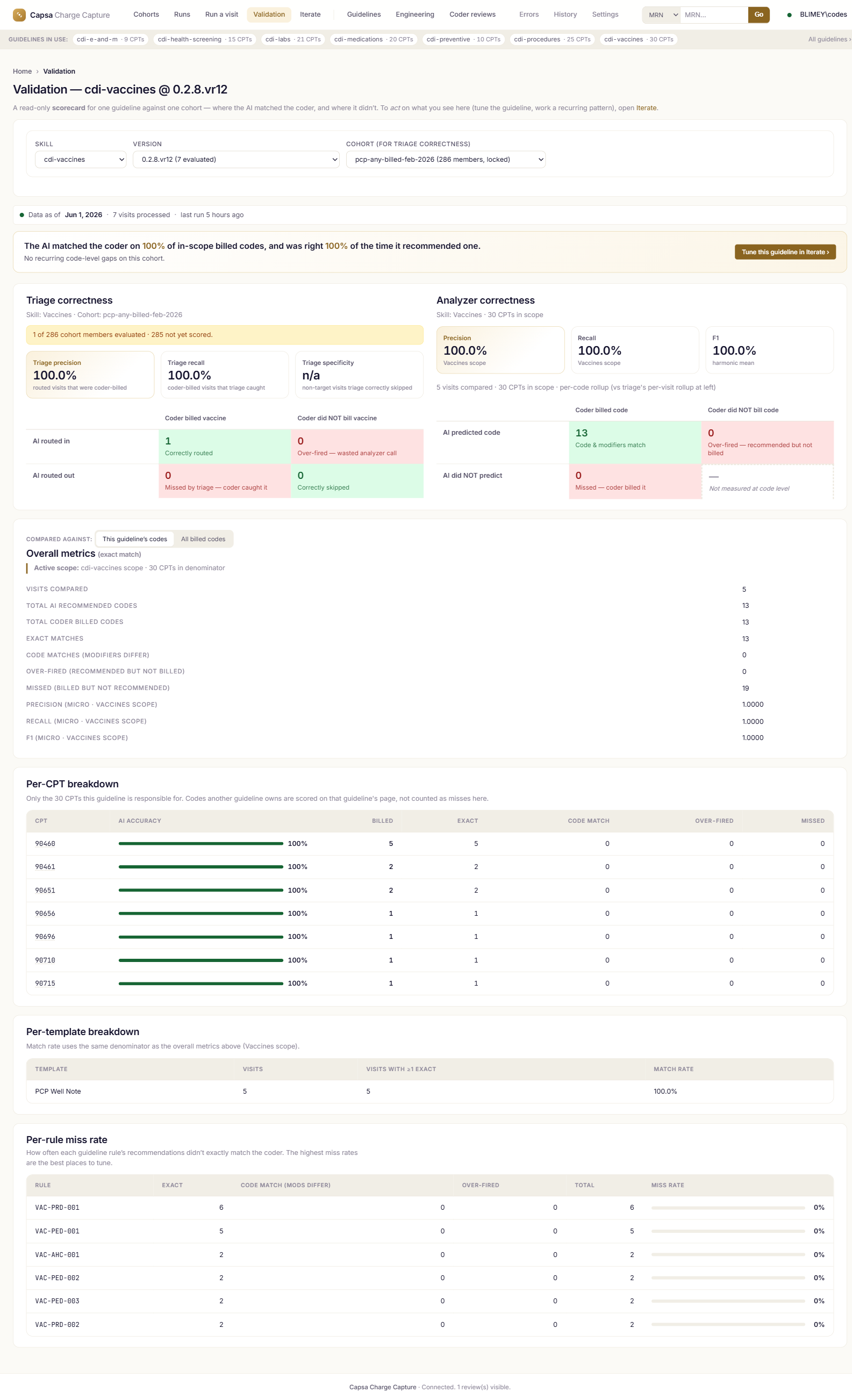
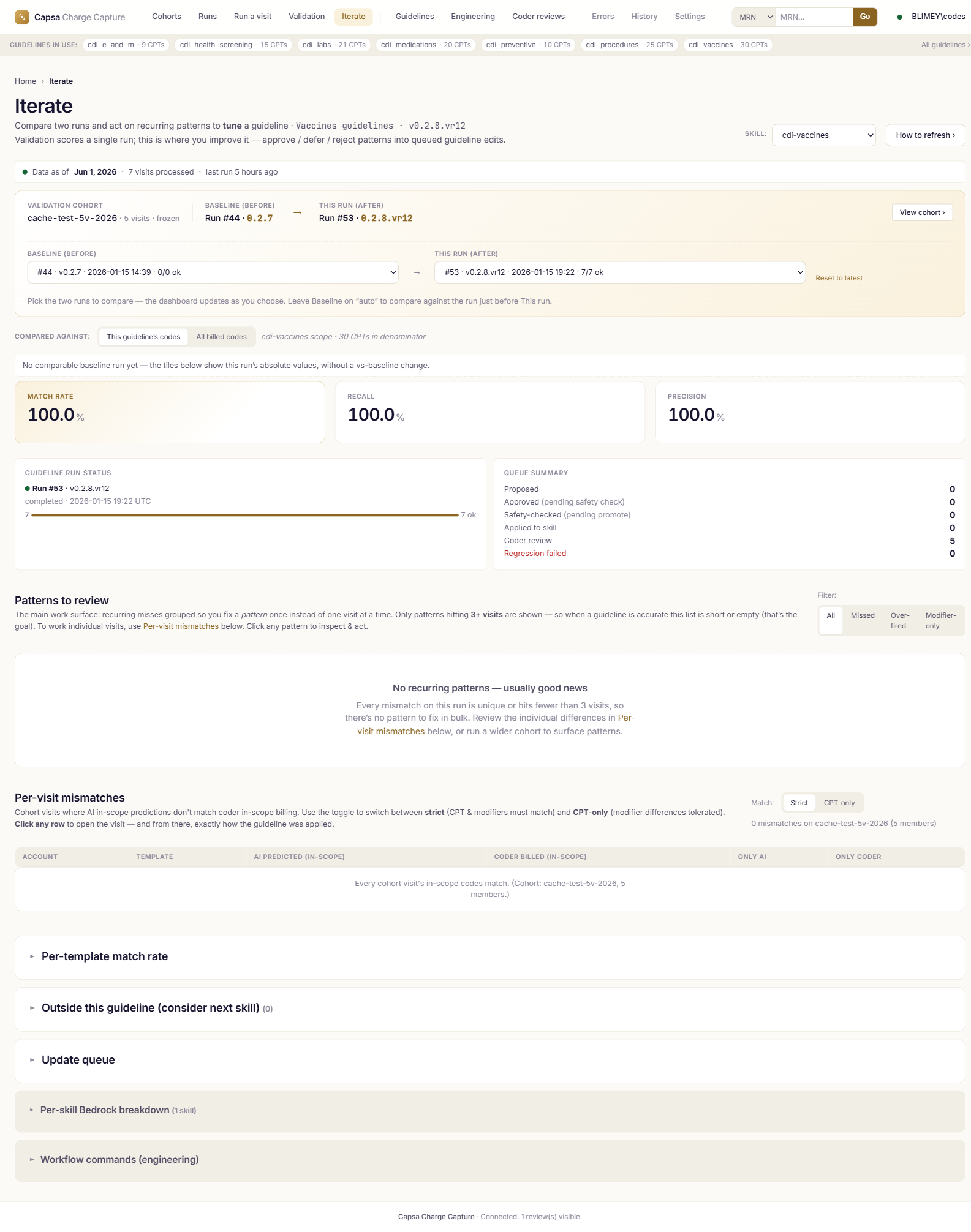
Measured on cases your team already coded.
Precision = of the codes Capsa recommends, the share coders agree with. Recall = of the in-scope codes coders billed, the share Capsa caught.
Two categories measured to date
Vaccines and health screening are measured and proven; five more categories are built on the same framework with measurement in progress.
| Coding category | Precision | Recall | Note |
|---|---|---|---|
| Vaccines | 96.9% | 95.5% | Recall SLA (≥95%) met; precision at target. |
| Health screening · A | 93.7% | 95.7% | Recall SLA met. |
| Health screening · B | 93.9% | 93.4% | Both metrics near target. |
Built to be defended in an audit — not just to find more codes.
Audit-defensible by design
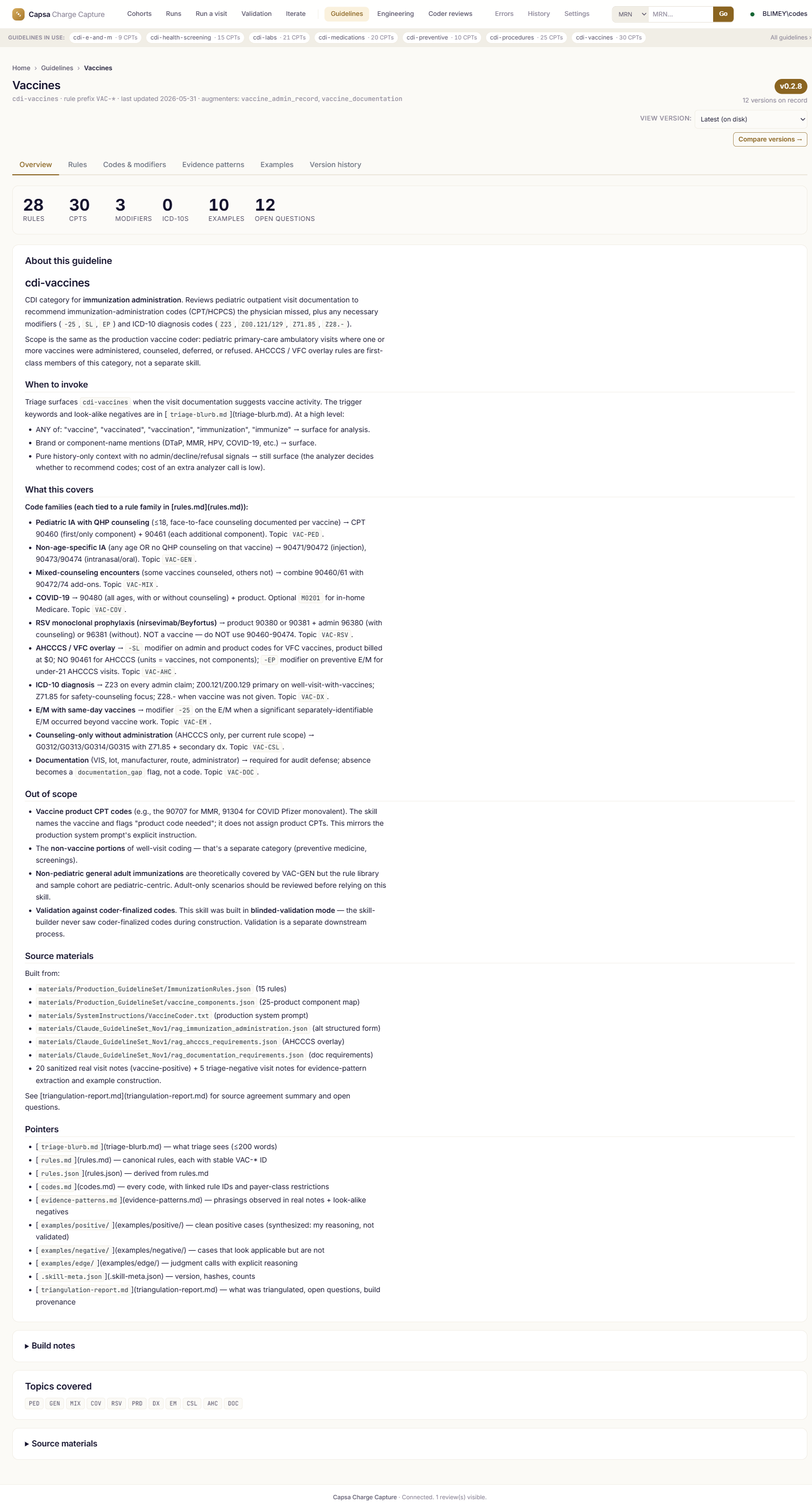
Every code links to the rule that produced it, and every rule to the verbatim chart text that triggered it — at the exact version that ran. Answer “why this code?” in one click.
Versioned guidelines
Rules, codes, evidence, and worked examples are versioned together with full history and side-by-side diffs. When a payer changes a rule, the change is on the record.
Scope-aware measurement
Precision and recall are measured against the codes each skill actually owns — so the numbers mean what they say instead of being diluted by out-of-scope codes.
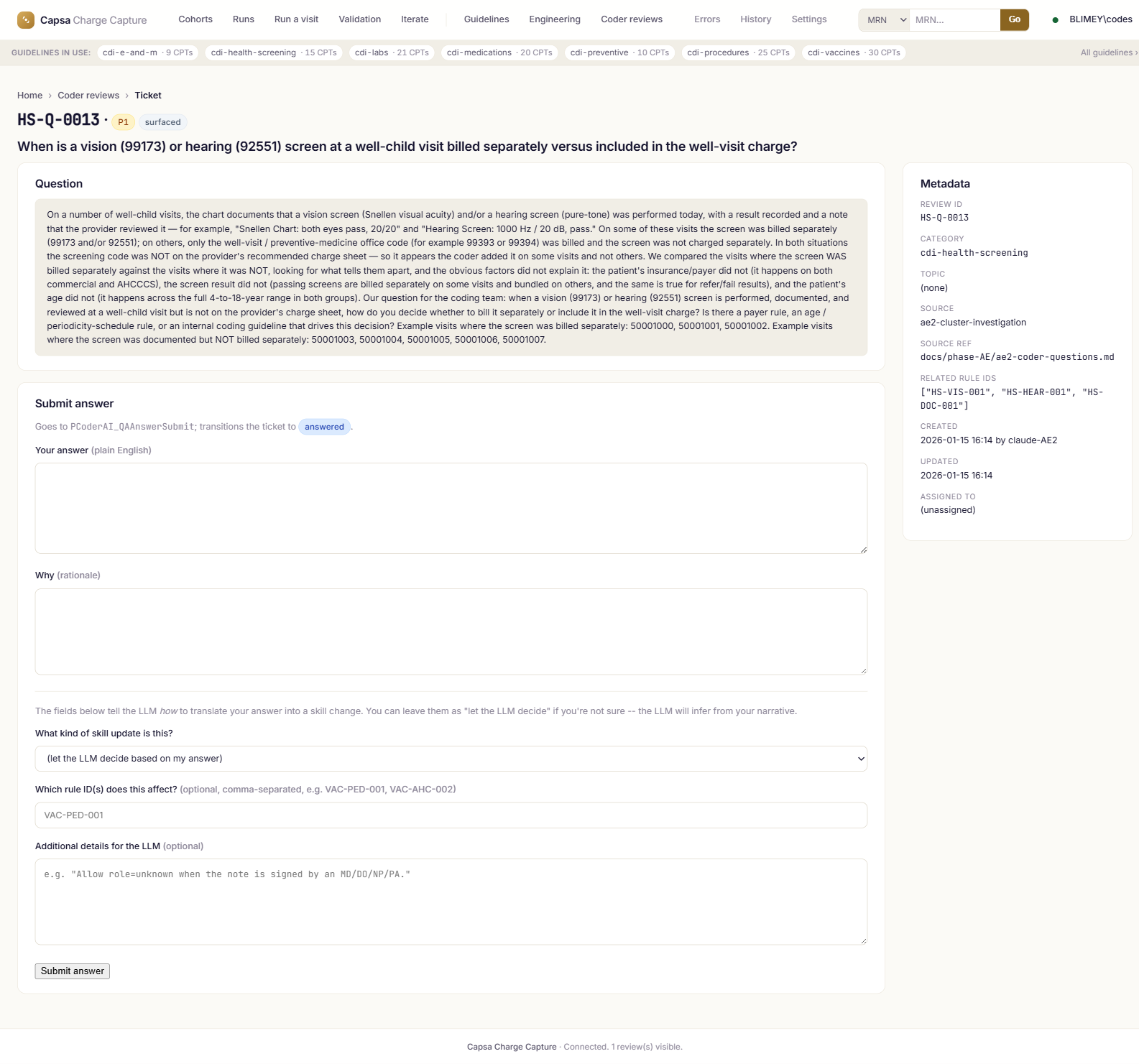
Clinician-governed loop
CDI nurses — not engineers — answer clarifying questions and approve rule updates through a guided workflow, with a complete audit trail.
No black box, no fine-tuning
All clinical logic lives in explicit, human-readable rule sets. Nothing is hidden inside a model nobody can inspect or explain.
One framework, every category
The same engine runs every coding skill. Adding a new category is reuse, not a rebuild.
See the whole loop, end to end.
The Capsa Charge Capture overview
A short walkthrough of ingest → triage → analyze → cite-check → validate, on real screens.
Video coming soon — book a pilot to see it live on your data Book a pilotQuestions coders, CDI, and compliance ask.
How is this different from a black-box coding model?+
Will Capsa replace our coders?+
How do you measure accuracy?+
Is it audit-defensible?+
What does a pilot involve?+
How do you handle PHI and data security?+
See Capsa on cases your team already coded.
We'll run Capsa Charge Capture against your guidelines, your cohorts, and your paid claims — and show you scope-aware precision and recall on visits you've already billed.
- Pilot on a sample of your own visits
- Precision & recall vs. what your coders billed
- Every recommendation cited to the chart
- No EHR rip-and-replace
Request a demo / pilot
We'll get back to you within one business day.